What is a horseshoe kidney?
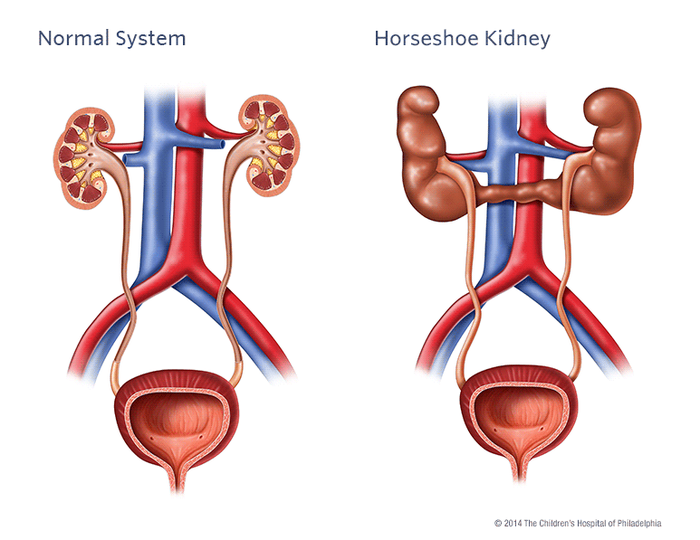
Most people have two separate kidneys which each have a single tube (ureter) that connects to the bladder. This tube drains urine from the kidney into the bladder from where you pass urine.
More about the urinary system.
In some pregnancies, the kidneys do not develop normally. One such variation is known as a horseshoe kidney.
A horseshoe kidney means that, instead of having two separate kidneys on each side of the body, the two kidneys are joined by their lower parts forming a U-shaped or horseshoe kidney.
Share this page with a QR code
Click on the blue box (on the right or below) and scan the QR code with your phone or tablet.

This web page is printer-friendly.
To save the page as a PDF, print as normal and select "Save as PDF" as your printer destination.