What is pelvi-ureteric junction (PUJ) dysfunction and obstruction?
Pelvi-ureteric junction (PUJ) dysfunction is a congenital anomaly of the kidneys and urinary tract.
In some children the urine that is made in the kidney is not able to drain into the bladder as quickly as it is produced. The affected kidney(s) become swollen and this swelling (dilatation) can be seen on ultrasound scans and is known as hydronephrosis. Urine drains from the kidney through a funnel shaped structure called the renal pelvis into a tube called the ureter then down into the bladder. A narrowing or blockage where renal pelvis meets the tube (ureter) is known as pelvi-ureteric junction (PUJ, or UPJ) dysfunction or obstruction.
The word ‘dysfunction’ is usually used to begin with, and the word ‘obstruction’ later if the narrowing gets worse and surgery is needed, but either may be used.
This swelling of the kidneys may be noticed on ultrasound scan during your pregnancy (antenatal hydronephrosis) and your baby may need further investigations after he / she is born. On other occasions it is not diagnosed until the baby has already been born, or, in rare cases it may be found in an older child.
About pelvi-ureteric junction dysfunction and obstruction
The PUJ is the area where the pelvis of the kidney joins the ureter.
PUJ dysfunction is one type of congenital renal anomaly:
- congenital – the problem is present at birth
- renal – to do with the kidneys
- anomaly – different from normal
In very rare circumstances, it may be acquired. This means that the child was not born with the problem but it developed over time.
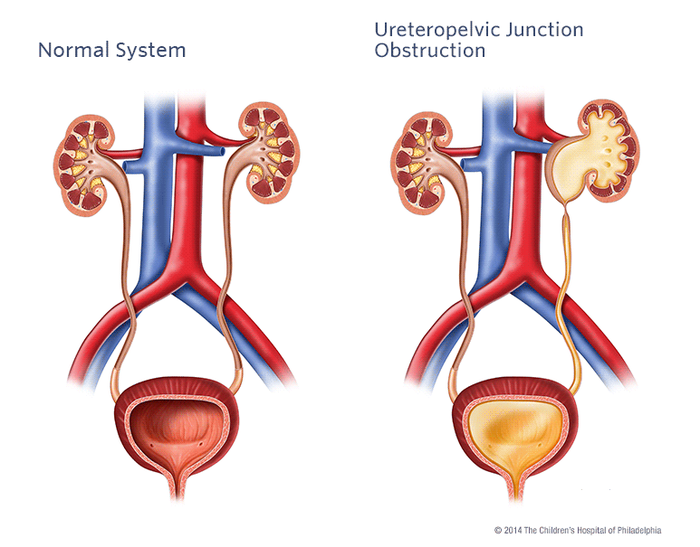
In PUJ dysfunction there is a narrowing at the point where the pelvis of the kidney joins the ureter. This stops urine draining normally from the kidney, down the ureter and into the bladder. This will result in a hold up of urine in the pelvis of the kidney, which becomes swollen. This is called hydronephrosis and is often first seen on an ultrasound scan, usually during pregnancy.
How does PUJ dysfunction happen?
As babies develop in the womb, a tube forms that connects their developing bladder to each kidney. These tubes will become the ureters. They should be hollow to allow urine to pass through them from the kidney down to the bladder, and they have a wall that is made of a type of muscle called smooth muscle.
Most commonly, PUJ obstruction happens because there is a problem with the development of the muscular wall of this tube and so part of the tube becomes very narrow. This narrowing causes a blockage. Rarely, this muscular tube is being compressed by something outside of it such as a blood vessel.
Does PUJ dysfunction affect how the kidneys work?
Usually not. In a small number of cases the swelling may increase the pressure in the kidney which could lead to kidney damage on the affected side unless surgery is performed. However, in most cases of PUJ dysfunction the swelling remains the same for many years without affecting kidney function, and in other cases it can completely resolve / get better on its own.
Most babies and children do not have any symptoms after birth. Some are at risk of:
Urinary tract infections
Symptoms can include fever, vomiting, pain on passing urine, abdominal or back pain, needing to pass urine more frequently.
Symptoms relating to obstruction to the flow of urine
Older children may rarely have these symptoms, which can include pain in the loin (side of the tummy) or blood in the urine (haematuria).
If you think that your child may have these symptoms, contact your doctor. If you cannot reach your doctor straight away, contact 111 or NHS Direct or your local out-of-hours GP service.
Diagnosis and tests in pregnancy
Most commonly, this problem is first detected during routine ultrasound scans in pregnancy. One or both of the baby’s kidneys may be noted to be swollen on those scans. There are, however, other causes of swollen kidneys and so your baby will need further tests to confirm the exact cause after they are born.
During routine scans, other things about your baby will also be monitored such as:
· How well he / she is growing
· How much fluid is around the baby
Other conditions that look like PUJ dysfunction
There are a number of other conditions that might cause hydronephrosis in a baby. These include:
Transient hydronephrosis
Most cases of antenatal hydronephrosis are not serious. The problem may disappear by the time the baby is born, or in the first year or so of life with no long-term effects on the baby
Vesicoureteral reflux
Urine travels back up the tubes from the bladder to the kidneys (it goes in the opposite direction it should do normally). This may be associated with symptoms of a urinary infection, bloody or cloudy urine.
Vesicoureteric junction Obstruction (VUJO)
In VUJO there is usually a narrow and stiff section of the ureter as it enters the bladder. This causes a hold up of urine passing into the bladder, causing a build-up in the ureter and kidney which become swollen.
Posterior urethral valves in boys
These are extra flaps of tissue in the tube that carries urine out of the body in males. Babies with PUV may not be able to wee normally – both while growing in the womb and after they are born
Other conditions that may be seen with PUJ dysfunction can be seen on its own or in combination with other problems include:
Horseshoe kidney
A horseshoe kidney means that, instead of having two separate kidneys on each side of the body the two kidneys are joined by their lower parts forming a U-shaped or horseshoe kidney
CHARGE syndrome
Children with a chromosomal (genetic) disorder called CHARGE syndrome can be more likely to have PUJ obstruction. If it is known that your child has this chromosomal (genetic) disorder or there are concerns that your child has an anomaly (difference) in another part of his / her body then, he / she may be referred to a geneticist. A geneticist is a doctor who specialises in genetic disorders.
Diagnosis and tests after birth
There are a number of tests that can be done to look at the structure of the kidneys and how well they are functioning. Your child may have some or all of the tests below.
Ultrasound
After your baby is born, he / she will normally have an ultrasound scan, similar to the ones done during your pregnancy. This may confirm that one or both kidneys are swollen but won’t generally confirm the exact cause. During this ultrasound, the person doing the scan will take some measurements of how swollen the kidney drainage systems are. These measurements may influence what type of scan your baby has next.
DMSA scan (Dimercaptosuccinic Acid)
This is a type of radionucleotide scan. This means that a substance that gives out a type of radiation called gamma rays is injected into the blood stream. This substance is taken up by the kidneys and a special camera takes some pictures. This allows us to see how well the kidneys are functioning.
MAG3 scan (mercaptoacetyltriglycine)
This is another type of radionucleotide scan. In this scan a substance called mercaptoacetyltriglycine is injected into the blood stream. It is also linked to a substance that gives out a type of radiation called gamma rays. It is taken up by the kidneys and then a special camera takes pictures. This type of scan gives us information on how well the kidneys are functioning, but also on how well urine is draining from the kidneys down into the bladder.
Urine tests
You, or a nurse, would need to collect some of your child’s urine in a small, clean container for a urine test. A dipstick will be dipped into the urine – this is a strip with chemical pads that change colour depending on what substances are in the urine. The sample may also be sent to a laboratory for more accurate tests.
Blood tests
As well as various scans, your child may have some blood tests. This gives an idea of how well the kidneys are working.
PUJ treatment before and after birth
In most cases, no treatment before birth is needed. The delivery may need to take place at a centre where urgent surgery could be undertaken if it were needed, but this is rarely required.
After birth
This depends on findings from the antenatal ultrasound scans and tests after birth. In most cases, babies can be discharged home a short time after birth. Rarely, babies need to be moved to a neonatal unit, an area of the hospital for newborn babies, for monitoring and treatment.
Preventing and treating urinary tract infections (UTIs)
Some babies may be at higher risk of urinary tract infections (UTIs). If your baby is found to have hydronephrosis during your pregnancy then after birth, he / she is likely to be prescribed some antibiotics. These are sometimes referred to as prophylactic antibiotics. This means that a low dose of antibiotic is given every day to prevent urine infections. These may be stopped later on the advice of your doctor if the scans that are done are reassuring.
Surgery
If the kidney scans show that the kidney is very swollen or not working well, then your child may be referred to a paediatric urologist (a surgeon specialising in operations on the urinary system in children). They will consider whether an operation called a pyeloplasty is needed. This operation may also be considered in older children if they have PUJ obstruction and have symptoms
A pyeloplasty is an operation performed under general anaesthetic to remove the narrowed PUJ and then connect the pelvis of the kidney back to the healthy ureter. The operation can either be done keyhole (laparoscopy) or with open surgery. Your surgeon will discuss with you, which method is most appropriate for your child.
In the future
Your child should be able to do all of the things that other children their age do. Your child should be able to go to nursery and school, play with other children and stay active.
Follow up
Your child will be followed up by healthcare professionals, usually at a hospital. This may be a paediatrician (a children’s doctor), a paediatric nephrologist (a specialist in kidney care) or a paediatric urologist. Your child will have regular monitoring scans, usually every 3-6 months over the first few years of life, although this may vary slightly in different hospitals.
Long-term effects
In most babies and children, the degree of swelling is mild, and doesn’t progress over the first few years of life. At this point, scans will stop and nothing will need to be done unless your child developed symptoms. A very small number of children develop long-term problems with their kidneys and will need specialist follow-up throughout life.
Will it happen in future pregnancies?
PUJ dysfunction is not a condition that is inherited. This means that it is unlikely that a future pregnancy will be affected. However, if you have any concerns then speak with your doctor for more information.
Further support
This can be a difficult and stressful experience for you and your family. If you have any concerns or need additional support, speak with your doctor or nurse.