Haemodialysis is an important treatment for kidney failure (when the kidneys stop working properly).
Using a special machine with an ‘artificial kidney’, haemodialysis removes extra water, salt and waste products from the blood.
Your child will need a procedure to get access to their bloodstream for haemodialysis. One option is to create a fistula.
What is a fistula?
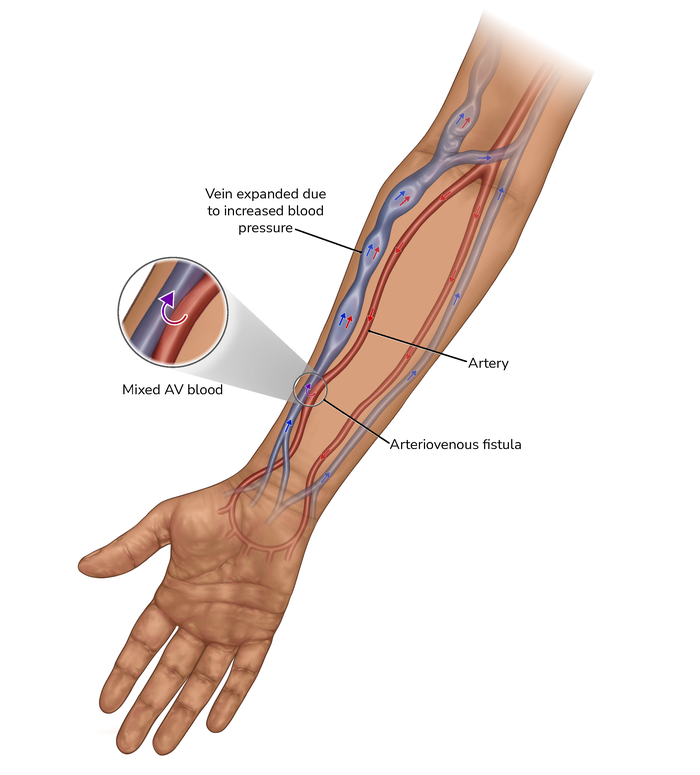
An arteriovenous fistula (usually shortened to AV fistula or fistula) can be formed in the arm. It joins two types of blood vessels – an artery (which carries blood from the heart round the body) and a vein (which carries blood back to the heart). This makes one large, stronger blood vessel. The blood carried through the artery can go straight into the vein.
The fistula is usually formed in the arm that your child does not draw or write with. It is one of two places:
- inside of the elbow (a brachiocephalic fistula or brachiobasilic fistula) – usually for younger children
- inside of the wrist (a radiocephalic fistula) – usually for older children and adults.
With a good functioning fistula there is a ‘buzzing’ feeling in the area (this is the effect of the blood passing through). Your child will be shown how to take care of their fistula.
How is a fistula used?
A fistula needs to be made about 8 weeks before dialysis starts, to allow time for it to develop and get strong enough.
For regular dialysis sessions, two needles are inserted into the fistula – because it is a larger, strong blood vessel, it is easier to access and remove blood. A special gel or cream can be put on your child’s skin to help your child stop feeling any pain when the needles are put in.
Why is a fistula recommended?
For many children, a fistula is the best option for access to the blood when haemodialysis is needed over a long time because there is much less risk of infection or blockage. Occasionally, a fistula fails to develop, or there is bleeding or other complications, and some children need to come back for a new procedure.
- A fistula is much less likely to become infected than a ‘line’. This is important because an infection can damage the lining of a blood vessel.
- A fistula also lasts for a longer time than a line. There are only four blood vessels that can be used to create a fistula. If these have all been used to form fistulae, your child may need to use a line instead.
Small children may not be ready for a fistula. They may need to have a central venous line for haemodialysis, until they are large enough for a fistula.
Central venous line: a haemodialysis access alternative to a fistula
The alternative to a fistula is a central venous line. This is a soft, long, thin tube (catheter) that is placed into one of the large blood vessels in your child’s body. This is usually in the neck or chest, or occasionally the groin. It is often called a ‘line’.
A temporary line can be placed for children who will need haemodialysis quickly or for a short time. For long-term use, a permanent line can be placed by surgery. For each dialysis session, tubes are connected to the end(s) of the catheter.
A line may be more suitable for, or preferred by, some children – especially those who are too small for a fistula. It does, however, have a greater risk of infection or blockage, and needs to be looked after carefully.
Share this page with a QR code, print or save as PDF
Click on the blue box (on the right or below) and scan the QR code with your phone or tablet.

This web page is printer-friendly.
To save the page as a PDF, print as normal and select "Save as PDF" as your printer destination.