Posterior urethral valves (PUV) are extra flaps of tissue in the back (posterior) part of the urethra. They develop while a baby boy is growing in the womb.
PUV are the most common type of bladder outlet obstruction in newborn babies. This means that they stop (obstruct) the flow of urine out of the bladder. PUV need to be removed by surgery.
PUV are rare. In the UK, it is estimated that around one newborn boy in 8,000 has PUV. It is not known why some boys have PUV. They are not inherited from either parent, or caused by anything that the mother does during her pregnancy.
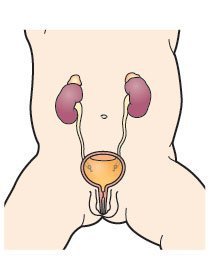
PUV may happen with other abnormalities in the urinary system. This may mean that one or both kidneys or ureters do not develop properly.
Will it affect other family members?
Doctors do not think that PUV runs in families. If one of your children has PUV, it is unlikely that another of your children or another family member will get them.
Share this page with a QR code, print or save as PDF
Click on the blue box (on the right or below) and scan the QR code with your phone or tablet.

This web page is printer-friendly.
To save the page as a PDF, print as normal and select "Save as PDF" as your printer destination.